
Loading Experience
Linked Patient Learning
Loading Experience
Rare disease companies invest heavily in patient engagement. You have dedicated patient services teams, hub services, specialty pharmacy partnerships, foundation coordination, field reimbursement support.
The investment is there. The commitment is real.
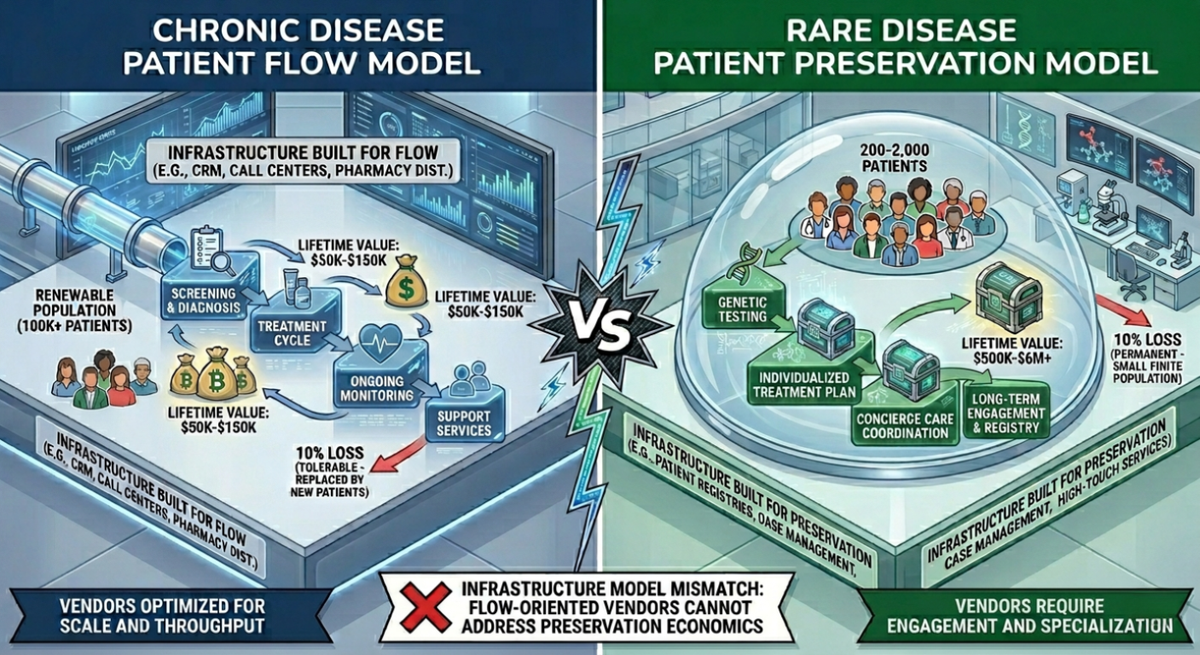
But here's the problem: Your patient engagement infrastructure follows an industry model designed around chronic disease assumptions—large, renewable patient populations with lower lifetime value.
In rare disease, the economics are fundamentally different:
Patient populations: 200 to 2,000 globally. Finite.
Patient lifetime value (LTV): $500K to $2M+. Sometimes $6M+.
Therapy duration: Life-long.
When a rare disease patient discontinues due to a coverage gap no one detected, you don't lose a prescription. You lose a seven-figure asset.
The question isn't whether you're investing in patient engagement. You are.
The question is whether your infrastructure is designed for rare disease economics—or following a model built for different assumptions.
Economics:
The chronic disease model is built around large, renewable patient populations—typically 100,000+ patients—with lifetime value (LTV) ranging from $50K to $150K per patient. In contrast, rare disease operates with small, finite populations of just 200 to 2,000 patients, where each patient represents $500K to $6M+ in lifetime value.
This economic difference fundamentally changes the math: When you lose 10% of patients in chronic disease, they're replaced by new patient enrollment, making the loss manageable. But in rare disease, losing 10% means permanently losing 10% of your entire market—there is no replacement pool. This reality makes the ROI on prevention 10 to 40 times higher in rare disease than in chronic disease.
Infrastructure Design:
Chronic disease infrastructure is vendor-optimized, meaning each vendor—hub, specialty pharmacy, foundation—optimizes their individual function. Gaps between vendors create inefficiency but are generally tolerable given the large patient populations. Rare disease, however, requires journey-optimized infrastructure where gaps between vendors translate directly to patients lost in handoffs that no single vendor owns.
The impact of this design mismatch is stark: 10 patients lost in infrastructure gaps within a 50,000-patient chronic disease population is unfortunate but survivable. Those same 10 patients lost within a 500-patient rare disease population represent 2% of the entire market and $20M to $60M in lost lifetime value.
Success Metrics:
Chronic disease infrastructure measures vendor performance—enrollment completion rates, benefit verification turnaround times, call resolution scores. These metrics track operational efficiency. Rare disease requires patient outcome metrics—discontinuation root cause analysis, coverage continuity tracking, lifetime value protected, and early intervention effectiveness.
The critical insight: Strong vendor performance metrics don't equal patient retention when the underlying infrastructure wasn't designed for journey continuity. You can have excellent vendor scorecards while patients discontinue in the gaps between those vendors—and in rare disease, each gap costs millions.
What the Numbers Don't Capture
Provider hesitation:
In chronic disease with 50,000 patients, a rheumatologist might have 200 on therapy. When 5 discontinue, it's unfortunate.
In rare disease with 500 patients globally, a specialist might have 8 patients total. When 2 discontinue due to coverage gaps your infrastructure didn't detect, they remember. They hesitate to start patient #9.
Patient community impact:
In chronic disease, patients don't know each other. One bad experience stays isolated.
In ultra-rare disease, patients know each other. Online communities. Annual conferences. Advocacy groups. When one patient loses coverage and discontinues after your infrastructure failed to detect the gap, other patients hear about it. Provider confidence erodes. Community trust weakens.
Your infrastructure failure doesn't just lose that patient's $2M LTV. It creates provider hesitation and community concern that compounds across your entire ultra-rare patient pool.
That's what vendor-optimized infrastructure misses.
What This Looks Like in Practice
You're doing everything right by chronic disease standards:
✓ Hub enrollment: 95% completion
✓ Benefit verification: 48-hour turnaround
✓ Specialty pharmacy: 87% first fill within 14 days
✓ Foundation: Average 21-day approval
✓ Patient satisfaction: Excellent scores
Then Month 8 happens:
Patient's Medicaid redetermination creates coverage gap. Foundation processing takes 18 days. Pharmacy can't fill without coverage. Hub doesn't monitor coverage between touchpoints.
Patient goes 3 weeks without therapy. Discontinues.
Your vendors all performed well. Your infrastructure failed.
LTV captured: $400K. LTV lost: $1.6M.
This isn't a vendor failure. It's a model mismatch. Your vendors were optimized for their functions. Your infrastructure wasn't designed for the patient's journey.
The 3 Infrastructure Must-Haves for Rare Disease
You're already investing in the 10%: Activation, enrollment, benefit verification, first fill.
The gap is the 90%: Three critical capabilities your current infrastructure likely lacks.
Cross-Ecosystem Visibility:
Current infrastructure operates with four separate vendor reports. Your hub shows enrollment data, your specialty pharmacy reports on fills, your foundation tracks approvals—but gaps between these vendors remain invisible. You're piecing together the patient journey from disconnected data sources, often discovering problems only after they've caused discontinuation.
The 90% Framework delivers a single patient timeline across all vendors. You see the complete journey: hub enrollment flowing to pharmacy fills, foundation applications processing, field reimbursement support activating—with every handoff visible in real-time. You know exactly where each patient is in their journey and can identify gaps as they emerge, not weeks later in retrospective analysis.
Proactive Coverage Monitoring:
Current infrastructure verifies coverage at enrollment and checks again when prior authorization is submitted. Coverage gaps are discovered post-facto—when the patient reports a problem or misses a fill. By then, therapy has already been interrupted and you're in reactive recovery mode.
The 90% Framework implements automated tracking of Medicaid redeterminations, ACA subsidy eligibility changes, and commercial insurance renewals. The system generates 30-day advance alerts before coverage gaps can cause discontinuation, enabling proactive bridge protocols and coordination to maintain therapeutic continuity rather than scrambling to recover patients already lost.
Early Intervention Protocols:
Current infrastructure relies on quarterly vendor scorecards and reactive outreach once patients have already missed fills. Post-mortem analysis after discontinuation reveals what went wrong, but the $2M patient is already gone. You're managing by lagging indicators.
The 90% Framework uses automated triggers that respond to patient signals in real-time. Coverage gap detected leads to intervention within 48 hours. Refill pattern changes trigger proactive outreach before discontinuation occurs. You're intervening based on early warning signals, not responding to failures that have already happened.
The outcome:
Current infrastructure: Patient discontinues Month 8. Post-mortem reveals Medicaid gap. Vendors performed to SLA. $1.6M lost.
90% infrastructure: Month 7, system detects upcoming redetermination. Proactive bridge coordinated. Patients maintain therapy. $2M protected.
Same vendors. Different orchestration.
The Rare Disease Reality
In chronic disease, you optimize for patient flow. New patients replace discontinued patients. Infrastructure inefficiency is tolerable.
In rare disease, you protect irreplaceable assets. There is no patient flow. There is patient preservation.
Your vendors were built for flow. Your economics require preservation.
The 90/10 Framework isn't about investing more in patient engagement. It's about investing differently—because in rare disease, infrastructure designed for renewable populations will destroy finite ones.
Linked Patient Learning helps rare disease pharma redesign patient engagement infrastructure around journey economics—not vendor benchmarks.
Schedule a Rare Disease Infrastructure Assessment: We'll map where your patients actually discontinue, quantify LTV at risk, and show the gap between your current vendor allocation and what your patient journey requires.
Written by
Liza Prettypaul-Lodhia
Share your details and we'll send you the playbook.