
Loading Experience
Linked Patient Learning
Loading Experience
Consider the math: A specialty brand with 2,000 patients on high-cost therapy.
If coverage churn causes even 10% to discontinue = massive revenue impact.
And your infrastructure can't detect coverage gaps until it's too late.
See the problem?
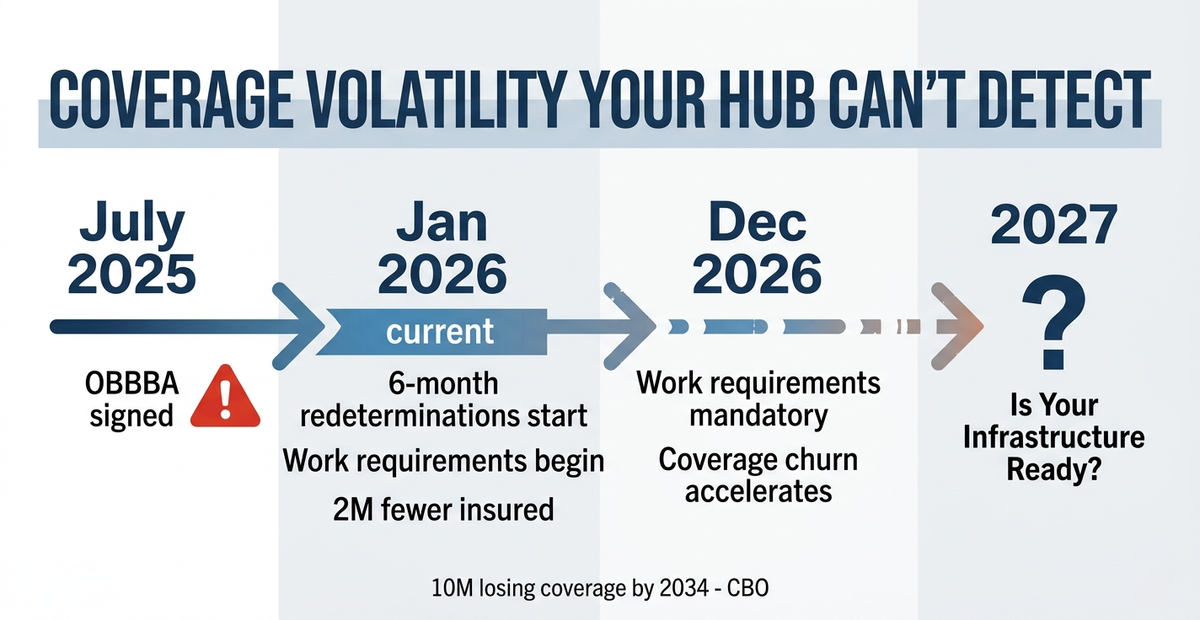
The One Big Beautiful Bill Act, signed in July 2025, will result in an estimated 10 million people losing health insurance coverage by 2034, according to the Congressional Budget Office. American Medical Association
For pharma patient support teams, this isn't a policy debate. It's an operational crisis with direct P&L impact.
What Changed in 2026
Starting January 2026, several provisions took effect: Medicaid work requirements begin implementation, six-month (versus annual) eligibility redeterminations, and elimination of income-based special enrollment periods for ACA marketplace premium tax credits. American Medical AssociationHealthInsurance.org
Enhanced ACA premium subsidies expired December 31, 2025, leaving an estimated 2 million fewer people insured in 2026. American Medical AssociationAl Jazeera
Translation: More patients will cycle in and out of coverage. More will face financial barriers mid-treatment. More will disappear from your systems during coverage gaps.
The 90% Just Got Harder
Your patient engagement infrastructure was designed for stable coverage and predictable touchpoints.
The One Big Beautiful Bill Act creates the opposite:
Coverage churn: Medicaid enrollees face more administrative hurdles when applying for or renewing coverage, with six-month redeterminations replacing annual reviews. HealthInsurance.org Patients who were stably insured will experience repeated coverage disruptions.
Financial complexity: Premium subsidies gone. Work requirements active. Patients choosing between employment and therapy access.
Rural access collapse: Hospitals are making cuts—closing maternity wards, shuttering community health centers, laying off staff—as they contend with both Medicaid cuts and reductions in provider taxes. CNN
What this could look like:
Rare disease patient, Month 8 on specialty therapy, clinically stable. Six-month Medicaid redetermination. Coverage lapses during processing. Your hub discovers it weeks later when prior authorization gets denied. Patient has been off therapy for a month. By the time coverage reinstates, they've discontinued. Your metrics show "patient non-adherence." Reality: infrastructure failure in the 90%.
The infrastructure problem: Your hub excels at benefit verification for newly enrolled patients (the 10%). But when coverage lapses mid-treatment, when patients lose eligibility during six-month redeterminations, when rural access points close—that happens in the 90%.
And most patient support infrastructure has zero visibility into it.
What This Actually Costs You
This isn't just a patient impact problem. It's a business model problem.
Revenue risk: For specialty therapies where annual treatment costs can range from tens to hundreds of thousands of dollars, coverage disruption mid-treatment compounds across your patient base. One coverage gap can end a long-term therapeutic relationship.
Competitive vulnerability: The pharma companies building infrastructure resilient to coverage disruption will demonstrate superior persistence rates. Those still optimized for stable enrollment will show declining outcomes—and struggle to explain why in payer negotiations.
Payer pressure: Value-based contracts require you to demonstrate therapeutic continuity and real-world persistence. When coverage volatility causes discontinuation, payers don't care that "it wasn't our fault." Your outcomes lag, your contract terms suffer.
Your metrics will lie to you: Patients discontinuing due to coverage gaps show up in your dashboard as "non-adherence" or "patient choice." Reality: system failure in the 90%.
Why Your Q2/Q3 Decisions Matter
Work requirements must be implemented by December 31, 2026, affecting Medicaid-eligible adults who must now meet community engagement mandates to maintain coverage. American Medical AssociationASTHO
Coverage churn accelerates through year-end as work requirements hit and six-month redeterminations cycle through.
If you're finalizing 2027 patient support budgets in Q2/Q3, the infrastructure you commit to now determines whether you can maintain therapeutic continuity through the disruption wave ahead.
The Strategic Question
10 million people losing coverage over the next decade means millions of specialty therapy patients will experience:
Your patient support infrastructure: Can it keep patients on therapy through these disruptions? Or does it only work when coverage is stable?
Most pharma built infrastructure for the 10% (stable enrollment, predictable benefits). The One Big Beautiful Bill Act just made the 90% (coverage disruptions, financial volatility, access barriers) the determining factor for persistence.
The companies redesigning infrastructure for this reality now will maintain therapeutic continuity and demonstrate outcomes through volatility.
Those waiting will watch patients discontinue due to coverage gaps their systems can't see or support.
Linked Patient Learning helps biopharma companies build patient engagement infrastructure resilient to coverage disruption—supporting the 90% where policy changes actually impact persistence.
Schedule a 30-minute Coverage Disruption Assessment:
We'll map where your infrastructure is blind to coverage gaps and show you the vulnerabilities most likely to cost you patients in 2027.
Written by
Linked Patient Learning
Share your details and we'll send you the playbook.